Do You Know The 5 Standards You Should Demand If Hospitalized With Parkinson’s?
By Michael S. Okun
Das Krankenhaus ist kein sicherer Ort, wenn Sie an Parkinson leiden. Jedes Jahr besteht eine 1:3-Chance, dass Sie als Parkinson-Patient ins Krankenhaus eingeliefert werden. Man würde erwarten, dass Sie nach einem Krankenhausaufenthalt schnell nach Hause entlassen werden und dass sich Ihre Parkinson-Symptome nicht verschlimmern. Die Realität sieht jedoch so aus, dass wir „unsere Sache schlecht machen“, wenn es darum geht, dieses Ergebnis zu erreichen. Eine große Gruppe von Kompetenzzentren im Netzwerk der Parkinson-Stiftung hat Artikel veröffentlicht und praktische Richtlinien, Kits und kürzlich ein Buch über die Sicherheit bei Krankenhausaufenthalten erstellt. Zuletzt haben sie einen wichtigen Kommentar im „Joint Commission Journal on Quality and Safety“ veröffentlicht. Die Autoren plädieren dafür, dass wir auf der Umsetzung und Durchsetzung von fünf Standards für die Krankenhausversorgung bestehen. In diesem Monat werden wir im Blog die Bedeutung der Sensibilisierung und der Erstellung eines proaktiven Plans für Krankenhausaufenthalte bei Parkinson-Erkrankungen erörtern.
Why do we care about preventing harm in hospitalized Parkinson’s folks?
Es gibt unverhältnismäßig viele vermeidbare und unbeabsichtigte Schäden in der Akutversorgung im Krankenhaus, unabhängig vom Grund der Einweisung. Zu den unerwünschten Folgen können gehören:
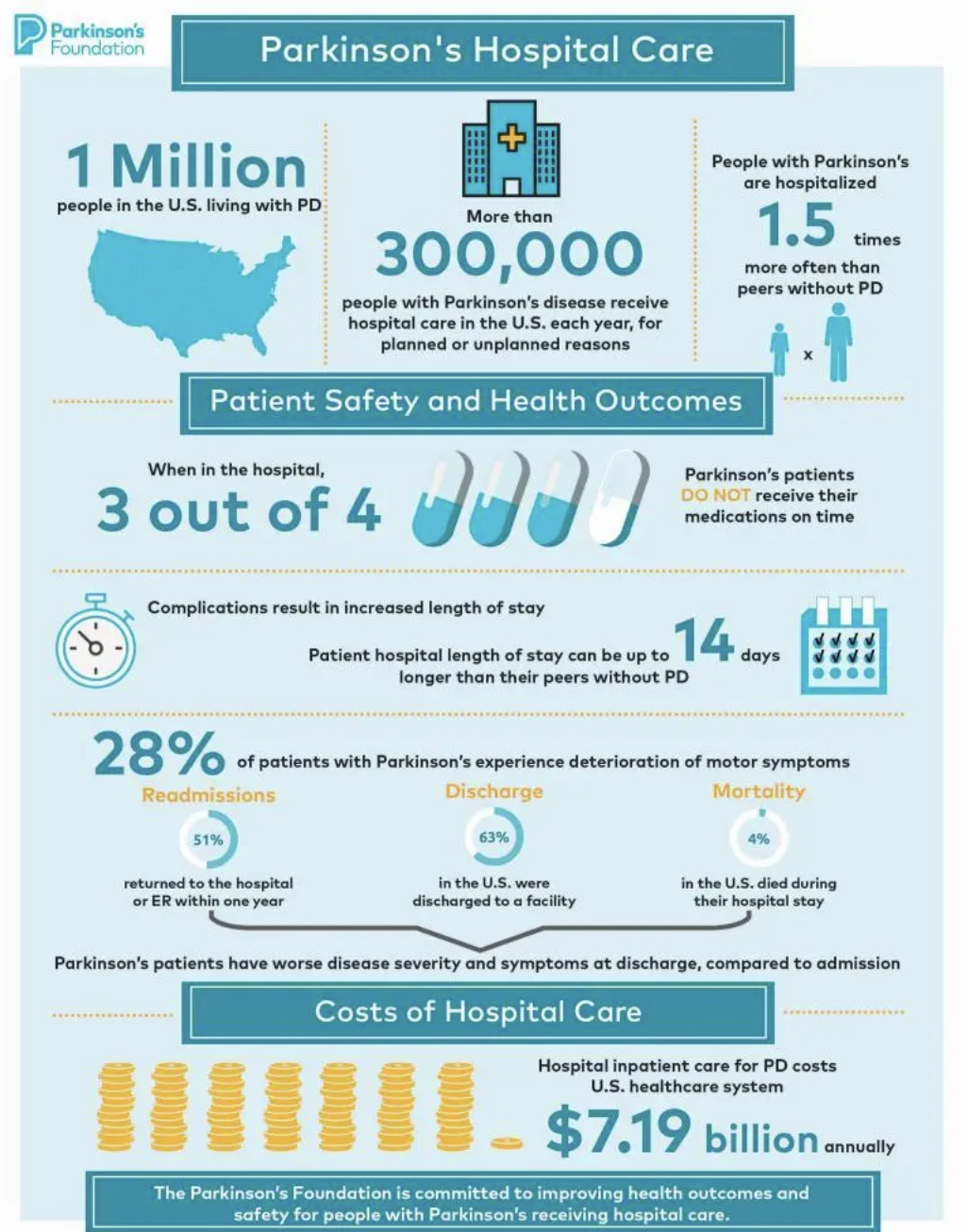
- Verschlechterung der motorischen Symptome bei 28 %
- Erhöhter Krankenhausaufenthalt von bis zu 14 Tagen länger
- Höhere Delirium-Raten von 11 % bis 60 %
- Höhere Sterblichkeit mit einer Sterblichkeitsrate von bis zu 3,8 bei Parkinson-Patienten im Vergleich zu Kontrollpersonen
- Parkinson-Patienten werden mit einer Wahrscheinlichkeit von 51 % innerhalb eines Jahres nach der Entlassung erneut eingewiesen
- Die Person würde mit einer Wahrscheinlichkeit von 62,9 % eher in eine andere Einrichtung als nach Hause entlassen
Why does the Joint Commission care so much about the hospitalized Parkinson’s person?
- Der Druck von politischen Entscheidungsträgern, Akkreditierungsstellen und Aufsichtsbehörden, die Patientensicherheit und -qualität zu verbessern, nimmt zu.
- Sicherheit und Qualität sind bei der Parkinson-Krankheit überproportional betroffen.
- Die Zentren für Medicare & Medicaid Services und die Joint Commission haben Qualitätsziele für Wiederaufnahmen festgelegt.
- Stürze sind bei Parkinson häufig, und Verletzungen werden als Sentinel-Ereignisse verfolgt. Diese sind bei Parkinson höher.
What are the current Parkinson’s Foundation hospital care recommendations?
- The Parkinson’s Foundation published (2023) the Parkinson’s Foundation Hospital Care Recommendations.
- There is now a systematic quality improvement framework which can be applied to improve hospital care.
What are the 5 recommendations you should insist on if hospitalized with Parkinson’s?
There are 5 hospital care standards that hospitals the author’s believe we must be meet to avoid preventable harm in Parkinson’s.
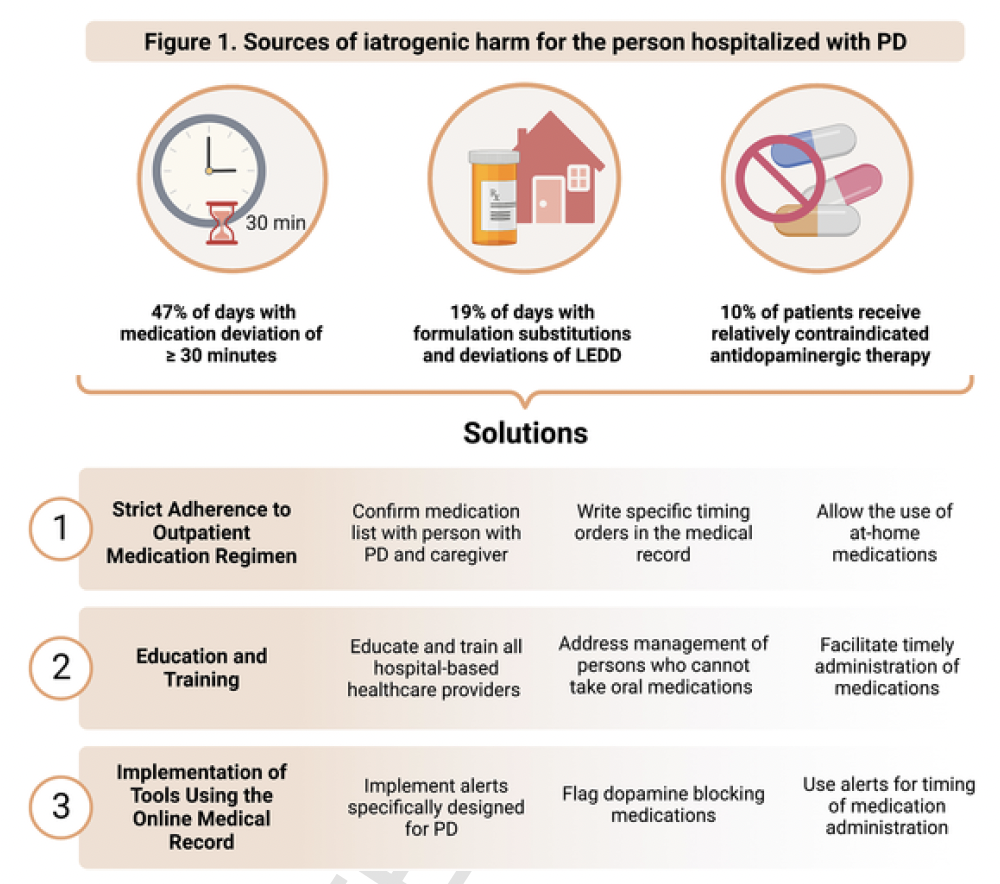
1. Alle Medikamente für die Parkinson-Krankheit werden individuell nach dem häuslichen Behandlungsplan der Patienten bestellt. Abweichungen von stabilen häuslichen Behandlungsplänen erhöhen bekanntermaßen das Risiko einer motorischen Verschlechterung, da die Halbwertszeit von dopaminergen Medikamenten kurz ist. Wenn sichergestellt wird, dass Ärzte stationäre Medikamente für die Parkinson-Krankheit individuell bestellen, wird sichergestellt, dass die Medikamente „jedes Mal pünktlich“ ankommen. Diese Praxis hat das Potenzial, die Aufenthaltsdauer zu verkürzen.
2. Alle Parkinson-Medikamente werden innerhalb von ± 15 Minuten nach dem Einnahmeplan zu Hause verabreicht. Dies sollte im Krankenhaus zu 100 % der Zeit erreicht werden. Eine frühzeitige oder verspätete Verabreichung von Medikamenten, selbst innerhalb von 30 oder 60 Minuten nach dem Einnahmeplan zu Hause, kann zu negativen Ergebnissen führen. Zwar gibt es nur wenige Belege für das genaue Zeitfenster, um Schäden zu verhindern, doch wird dieses Fenster mit fortschreitender Krankheit immer kleiner und die Dosierung muss häufiger erfolgen.
3. Schädliche Medikationsereignisse werden eliminiert. Der Fokus sollte auf Dopamin-blockierenden Medikamenten, Schmerzmitteln und Beruhigungsmitteln liegen. Häufig kontraindizierte (nicht einzunehmende) Medikamente wie Haloperidol, Metoclopramid und Prochlorperazin müssen vermieden werden. Es gibt auch Medikamente, die nicht per Definition kontraindiziert sind oder in den üblichen elektronischen Warnmeldungen für Krankenakten nicht aufgeführt sind, aber dennoch schädlich sein können.
4. Mobilisieren Sie dreimal täglich, wenn dies klinisch angemessen ist, und unter professioneller Aufsicht. Es gibt nur begrenzte Erkenntnisse über die genaue Menge oder Art der Mobilisierung, die erforderlich ist, um Schäden zu verhindern. Es besteht jedoch Einigkeit darüber, dass eine frühzeitige Mobilisierung entscheidend ist, um Komplikationen zu vermeiden.
5. Untersuchung auf Dysphagie (Schluckstörung) innerhalb von 24 Stunden. Dadurch kann das Risiko einer Aspirationspneumonie minimiert werden. Die Sterblichkeitsrate im Zusammenhang mit einer Aspirationspneumonie im Krankenhaus ist hoch (25 %).
How can hospitals and groups implement these changes?

The new guidelines suggest use of an implementation management system.
- The first step is preparatory, convening a multidisciplinary working group and clinical quality champions to drive change and to use the electronic medical record.
- The second step determines the initial scale of implementation (e.g., within a single unit, a single hospital, or multiple hospitals in a health system or hospital of a health system) and also the tactics.
- The final step should expand implementation beyond initial tactics.
What are some tips or tactics for improvement and implementation?
- Order medications in a custom fashion
- Determine a persons’ at-home regimen and consequences of delayed medication upon admission as part of the medication reconciliation process
- Enable a custom input for medications to align with at-home regimens rather than use default medication schedules
- Improve hospital-wide awareness of preventable harm through aggressive programs.
- Administer medications within ± 15 min of patients’ at-home regimen
- Implement data collection and review mechanisms that track and assess the discrepancy between patients’ at-home regimen and in-hospital medication administration
- Implement standard processes for reducing delays in medication administration.
- Avoid unnecessary orders on not take anything by mouth (NPO)
- Identify potentially contraindicated or potentially harmful medications.
- Use electronic health records based safeguard to avoid the prescription and administration of contraindicated medications
- Avoid inappropriate treatment of psychosis, confusion, or delirium with contraindicated antipsychotics
- Avoid contraindicated nausea/GI medications prescribed as part of standard postoperative care
- Avoid unnecessary medication substitutions
- Mobilize people with PD 3 times a day in the hospital
- Provide opportunities for patients to move safely and frequently in the hospital environment
- Provide Physical Therapy (PT) and occupational therapy (OT) orders
- Provide opportunities for communication and collaboration regarding patient mobility
- Screen for dysphagia within 24 hours
- Establish a standard protocol for screening of swallowing abilities
- Establish a protocol for minimizing the risk of aspiration pneumonia
- Establish a protocol for medication management in people with Parkinson’s experiencing varying degrees of dysphagia that prioritizes the closest adherence to their home medication regimen as is possible
Does the use of custom orders in the chart matter?
Researchers from Hackensack University Medical Center published a study in December 2023 that evaluated over 31,000 PD medication orders and determined that custom orders were more likely to result in timely medication administration when compared to non-custom orders.
Researchers from the University of Rochester published a study evaluating the impact of a best practice advisory (BPA) on contraindicated medications and determined that both contraindicated medication orders and administrations were reduced after implementation.
Researchers from Cleveland Clinic published findings from a study looking at the impact of changes in dosing and timing of medications from the stable home regimen. They showed a significant increase in length of stay, readmission, and death. This group of authors reminded us of the importance of utilizing drug-disease interaction alerts.
Finally there is a Parkinson’s Foundation Hospital Care Learning Collaborative with two dozen hospitals and health systems of varying size and complexity committed to sharing, implementing, testing, and refining best practices .
What is the bottom-line take home message
If you are planning a hospitalization or end up with an unplanned hospitalization then remember to insist on these 5 items:
1. Order medications in a custom fashion using the at-home regimen.
2. Administered medications within ± 15 min of a persons’ at-home regimen.
3. Do not use dopamine-blocking medications, pain medications, and sedatives which can worsen Parkinson’s.
4. Mobilize 3 times a day in the hospital.
5. Screen for swallowing within 24 hours of the hospitalization.
Now close your eyes and imagine if we did these 5 things consistently how much we could improve outcomes from hospitalization in Parkinson’s disease.


Selected references:
Azmi H, Walter BL, Brooks A, Richard IH, Amodeo K, Okun MS. Editorial: Hospitalization and Parkinson’s disease: safety, quality and outcomes. Front Aging Neurosci. 2024 Apr 4;16:1398947. doi: 10.3389/fnagi.2024.1398947. PMID: 38638192; PMCID: PMC11024459.
Veilleux Carpentier A, Salloum RG, Okun MS. Practical proactive and preventative Parkinson’s disease strategies for management in the hospital setting. Parkinsonism Relat Disord. 2023 Aug;113:105515. doi: 10.1016/j.parkreldis.2023.105515. Epub 2023 Jul 4. PMID: 37453869.
Shahgholi L, De Jesus S, Wu SS, Pei Q, Hassan A, Armstrong MJ, Martinez-Ramirez D, Schmidt P, Okun MS. Hospitalization and rehospitalization in Parkinson disease patients: Data from the National Parkinson Foundation Centers of Excellence. PLoS One. 2017 Jul 6;12(7):e0180425. doi: 10.1371/journal.pone.0180425. PMID: 28683150; PMCID: PMC5500337.
Zeldenrust F, Lidstone S, Wu S, Okun MS, Cubillos F, Beck J, Davis T, Lyons K, Nelson E, Rafferty M, Schmidt P, Dai Y, Marras C. Variations in hospitalization rates across Parkinson’s Foundation Centers of Excellence. Parkinsonism Relat Disord. 2020 Dec;81:123-128. doi: 10.1016/j.parkreldis.2020.09.006. Epub 2020 Oct 3. PMID: 33120073.
Chou KL, Zamudio J, Schmidt P, Price CC, Parashos SA, Bloem BR, Lyons KE, Christine CW, Pahwa R, Bodis-Wollner I, Oertel WH, Suchowersky O, Aminoff MJ, Malaty IA, Friedman JH, Okun MS. Hospitalization in Parkinson disease: a survey of National Parkinson Foundation Centers. Parkinsonism Relat Disord. 2011 Jul;17(6):440-5. doi: 10.1016/j.parkreldis.2011.03.002. Epub 2011 Apr 1. PMID: 21458353; PMCID: PMC3895941.
Hassan A, Wu SS, Schmidt P, Dai Y, Simuni T, Giladi N, Bloem BR, Malaty IA, Okun MS; NPF-QII Investigators. High rates and the risk factors for emergency room visits and hospitalization in Parkinson’s disease. Parkinsonism Relat Disord. 2013 Nov;19(11):949-54. doi: 10.1016/j.parkreldis.2013.06.006. Epub 2013 Jul 5. PMID: 23835430.
Aminoff MJ, Christine CW, Friedman JH, Chou KL, Lyons KE, Pahwa R, Bloem BR, Parashos SA, Price CC, Malaty IA, Iansek R, Bodis-Wollner I, Suchowersky O, Oertel WH, Zamudio J, Oberdorf J, Schmidt P, Okun MS; National Parkinson Foundation Working Group on Hospitalization in Parkinson’s Disease. Management of the hospitalized patient with Parkinson’s disease: current state of the field and need for guidelines. Parkinsonism Relat Disord. 2011 Mar;17(3):139-45. doi: 10.1016/j.parkreldis.2010.11.009. Epub 2010 Dec 14. PMID: 21159538; PMCID: PMC3070297.
Yu JRT, Sonneborn C, Hogue O, Ghosh D, Brooks A, Liao J, Fernandez HH, Shaffer S, Sperling SA, Walter BL. Establishing a framework for quality of inpatient care for Parkinson’s disease: A study on inpatient medication administration. Parkinsonism Relat Disord. 2023 Aug;113:105491. doi: 10.1016/j.parkreldis.2023.105491. Epub 2023 Jul 7. PMID: 37495500.
Azmi H, Cocoziello L, Harvey R, McGee M, Desai N, Thomas J, Jacob B, Rocco A, Keating K, Thomas FP. Development of a Joint Commission Disease-Specific Care Certification Program for Parkinson Disease in an Acute Care Hospital. J Neurosci Nurs. 2019 Dec;51(6):313-319. doi: 10.1097/JNN.0000000000000472. PMID: 31626076.
Bobek M, Pascarelli P, Cocoziello L, Azmi H. Utilizing the Nursing Professional Development Model to create and sustain nursing education aimed at improving the care of patients with Parkinson’s Disease in the hospital. Front Med (Lausanne). 2024 Jan 24;10:1275970. doi: 10.3389/fmed.2023.1275970. PMID: 38327273; PMCID: PMC10847593.
Azmi H, Cocoziello L, Nyirenda T, Douglas C, Jacob B, Thomas J, Cricco D, Finnerty G, Sommer K, Rocco A, Thomas R, Roth P, Thomas FP. Adherence to a strict medication protocol can reduce length of stay in hospitalized patients with Parkinson’s Disease. Clin Park Relat Disord. 2020 Oct 16;3:100076. doi: 10.1016/j.prdoa.2020.100076. PMID: 34316654; PMCID: PMC8298768.
